Join IHS in creating awareness of Medication-Overuse Headache. Share our videos in your social networks.
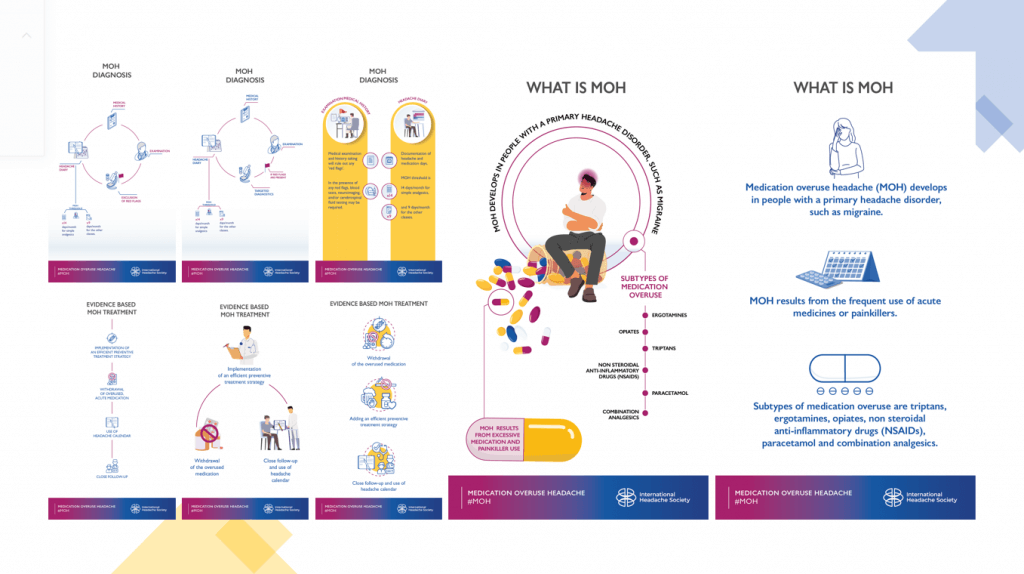
What is Medication-Overuse headache?
Almost all of us have headache sometimes, tension-type headache or migraine being the most common. Some unfortunately experience a gradually worsening headache despite an increasing use of painkillers. Understandably, this may lead to an extremely frustrating situation. On top of a worsening headache, medication and other strategies that previously helped, do not work as well any more – everything tried to relieve the headache seems to make it worse. This is the experience of patients who develop medication-overuse headache or MOH. Though not as common as migraine or tension-type headache, MOH is, the most common chronic headache type. The down-going spiral often becomes exceedingly burdensome also psychologically and adds to the general burden of a stressful every day and work-life.
This situation is difficult for patients to understand – it seems the headache has a “life of its own” even if handled in a way that has worked before and often, in a way that has been recommended by the treating physician. How previously well-functioning medication may contribute to maintenance of headache is indeed difficult to understand and requires awareness of the process and looking not just at the headache, but also at how the medication is used. Taking one step back and keeping track of how “at need” pain-killers are used is not easy. Patients are often aware of their medication not working as well as before but still feel that they have to take something. Some are worried about a high medication intake and have even tried to reduce their medication, often resulting in a worsening headache and thus suggesting the need to continue frequent intake. This behaviour has some similarity to addiction though it is not always easy to say if the increasing pain is driving the medication use or vice versa.
MOH develops in parallel with an increasing sensitivity also for other causes of headache and contributing factors. In addition general sensitivity for pain often increases in other parts of the body such as neck, shoulders and back, which may then contribute to frequent analgesics intake. This phenomenon of increased sensitivity to pain has been demonstrated in a number of studies in patients with MOH compared to other headaches without medication-overuse. The headache characteristics usually change over time as MOH develops. Headaches may be more un-relenting, continuous, and similar to tension-type headaches rather than the more attack wise, severe migrainous headache. However, MOH may also develop from episodic tension-type headache and in this case some headache days may become more migraine-like. This emphasises the difficulty in diagnosing the underlying, primary, headache.
There is a clear link between the medication overuse and the headache, demonstrated by the fact that headache usually improves if the patient is able to stop overusing acute painkillers. Unfortunately, an initial worsening of headache commonly occurs, for many providing “proof” that they should not stop analgesics intake. This rebound headache rarely extends over more than a few weeks.
Diagnosis of Medication-Overuse Headache
MOH is a dynamic disease that evolves over time, typically over years, in patients with a pre-existing headache with an episodic pattern, in most cases represented by migraine. The chain of events includes a worsening of frequency and/or severity of primary headache attacks over months/years paralleled by a progressively increased use of acute medications, until the threshold for chronicity (at least 15 headache days/month) and days of acute medication use (see table) is reached and maintained for at least 3 months.
The diagnosis of MOH therefore requires a careful history. A thorough examination is also necessary to exclude ‘red flags’, since multiple concurrent diseases may negatively affect the course of a pre-existing primary headache and prompt an increased use of acute medications. In the presence of any red flags, targeted diagnostic evaluation with blood tests, neuroimaging, and/or cerebrospinal fluid testing may be required. Another tool extremely important for diagnosing MOH is a headache diary or calendar, where the patient has to input the headache days and the days of use of acute medications. The diagnostic criteria of the International Classification of Headache Disorders (3rd edition) for MOH, which are shown here, are very simple and almost purely mathematical in their application.
The classification identifies multiple subtypes of medication overuse: simple analgesics, ergotamine, triptans, opioids or their combinations. The threshold for monthly days of use is set at 15 days/month for simple analgesics, while it is lowered to 10 days for the other classes. The diagnostic criteria do not consider the medication dosage per day, as reliable evidence is lacking in this regard.
Individuals receive a diagnosis of MOH along with the pre-existing headache diagnosis, usually migraine, less frequently tension-type headache, occasionally other headache types.
MOH diagnostic criteria have an inner limitation as they do not specifically mention the concept of temporal correlation between the increased use of acute medications and the worsening of headache frequency. While this correlation almost totally relies on patient’s recall, with the attached bias, it should always be searched by the clinician with an accurate history taking and, possibly, via health records or claims. Its presence substantiated the correcteness of the diagnosis and clearly informs the treatment approach whose first and main step is patient’s education about the offending action of overused acute medications.
Treatment of Medication-Overuse Headache
MOH is per definition an inappropriately treated headache. Therefore, treatment of MOH, can be viewed as an adjustment of the treatment towards a more efficient and optimal headache treatment.
Evidence based treatment of MOH consists of three elements: 1) Withdrawal of the overused and inefficient acute medication; 2) Adding an efficient preventive treatment strategy; and 3) Close follow-up and use of headache calendar.
This approach has shown to reduce headache days per month by fifty percentage; and about 70% of patients revert to an episodic headache form, meaning maximum 14 days per month with headache. Also, disability is decreased, and quality of life is increased. So, let’s have a more detailed look at each element in the MOH treatment strategy.
Withdrawal
When talking about withdrawal, the most efficient way, is to be without any painkillers or acute migraine medication for two months. Another approach, though less efficient in reducing the headache burden, would be to cut down the use of acute medication to maximum two days a week.
The most important issue of the withdrawal is to prepare the patient. That means providing detailed information about the nature of MOH, the reasons for withdrawing, and about the withdrawal procedure and potential withdrawal symptoms. Many patients may experience transient worsening in headache, but can be relieved by rescue medication, e.g., sedative drugs, antiemetics, prednisone, nonsteroidal anti-inflammatory drugs and so on. Normally, the headache and withdrawal symptoms will decline over the first 2-3 weeks. If possible, patients should consider sick leave in these weeks.
Specialized care should be considered, if patients are overusing opioids, barbiturates, benzodiazepines, or in case of considerable co-morbidities, or previously failed withdrawal.
Preventive treatment
Early start of preventive headache treatment in combination with withdrawal is recommended. The preventive treatment should target the pre-existing headache. If the pre-existing headache diagnosis is too unclear, the start of preventives may be delayed to after withdrawal.
Close follow-up and use of headache calendar
In line with detailed information, close follow-up and support of patients are essential for succeeding MOH treatment. Most patients relapse into a new MOH within the first year.
Moreover, headache calendar is recommended as an important tool for prevention and monitoring treatment.
So, to sum up, patients with MOH should start withdrawal therapy, start effective preventive treatment, and be offered close follow-up to prevent relapse. Thank you very much for your attention.
Medication-Overuse Headache Campaign
The IHS Education and Communications Committees are proud to present this Medication-Overuse Headache Awareness Campaign.
The IHS Medication-Overuse Headache Awareness Campaign focuses on educating Healthcare Professionals, offering the essential information to assist them in managing patients with tension-type headache.
In this campaign IHS members present short videos in their own languages on ‘What is medication-overuse headache’, ‘How to diagnose medication-overuse headache’ and ‘How to treat medication-overuse headache’. The content behind these videos was developed to raise awareness and promote education amongst clinicians and healthcare professionals worldwide on medication-overuse headache and its treatment.
The core message was developed in collaboration with Professors Cristina Tassorelli, Gisela Terwindt, and Christofer Lundgren, Dr Louise Carlsen, and Professor Rigmor Jensen, in collaboration with the IHS Education Committee. We greatly appreciate all IHS members who have been involved, and who have worked so hard to make this project possible. Help us spread the word
Healthcare Professionals play a vital role in medication-overuse headache advocacy and awareness efforts. By raising awareness within the medical community and increasing educational opportunities across the world, IHS aims to have a real impact on the lives of people with medication-overuse headache.
Please use #MOH2023 in all your posts.
Share amongst your colleagues and in your social media channels the educational videos we prepared in different languages, available on the IHS YouTube channel. Follow us in social media and subscribe to our YouTube channel for more updates on tension-type headache and other educational activities.
Medication-Overuse Headache Awareness Campaign videos
Videos in Spanish, French, Italian, Portuguese, and Arabic can be viewed on the IHS YouTube channel.
What is medication-overuse headache?
How to diagnose medication-overuse headache
How to treat medication-overuse headache
Please share these videos in your network and remember to use #MOH2023 in all your posts and direct your followers to the IHS social media channels.
You can also download infographics from our Google Drive.